Breathing Could Help You To Lose Weight!
Seeing as breathing is such a vital and fundamental part of our lives, one might think that we do it correctly, however we often don't. We tend to take shallow breaths and hold our breaths when focusing or under pressure. This lowers our oxygen levels causing fatigue and a lack of clarity and we can make poor decisions and perform poorly as a result. Sitting still in an office chair can also create an oxygen deficit and it is the reason why after vegging-out in front of the TV we feel exhausted even though we haven't done anything strenuous.
Oxygen thins the blood slightly which helps to lower your blood pressure and speed up the blood flow. This increases your metabolism and burns more calories, therefore the more oxygen you have in your blood, the faster your metabolism will be. You also burn more calories sitting outside than you do sat indoors, as cool air increases your metabolism as it tries to expend more energy keeping your body at a comfortable temperature. Therefore it is more beneficial to exercise outside than indoors.
If you're unable to exercise then deep, active breathing for a couple of minutes a day can increase your oxygen intake, reduce stress, strengthen muscles and burn more calories.
Also oxygen helps to break down fat molecules and the blood then picks up the waste carbon dioxide to transport it out of the body via the lungs, therefore the more oxygen we take in, the more fat molecules that can be burned off.
'Oxycise' is the latest weight loss programme sweeping across America claiming to transform body shape, shed pounds, improve muscle tone and boost energy level based on the information above. Instead of doing high impact aerobic exercise, Oxycise breathing techniques can be done anywhere. The deep breathing forces us to use more of our lungs, to tighten and strengthen the diaphragm muscles which makes our muscles contract and combined with some gentle exercises can burn fat and tone up muscles. A study even found that a women burned 140% more calories than riding an exercise bike.
However sceptics say that breathing too deeply is harmful as it can 'disturb the balance between carbon dioxide and oxygen needed to neutralise the blood and can cause light headiness and fainting' and that deep breathing is not going to burn enough calories to transform body shape, it may burn up 2% fat at best, Prof McDonald states.
The jury's still out without more detailed studies and research but it's an idea to definitely think about as it is such an easy technique that we can all do.
References: http://www.womensperfectbody.com and http://www.dailymail.co.uk

Tips For The Use Of Supplemental Oxygen
10 tips for using medical oxygen
If you require additional oxygen at home, you can improve your health by using the helpful advice listed below.
1. Make your home your first floor. Choose a bedroom on the first floor if you're moving or have the option to change how your house is set up, as climbing stairs is a fantastic form of exercise.
2. Get secure footwear. For both lounging around the house and working out, lace-up shoes that are supportive and comfy are a wise investment. Put on a shoe that will support your joints and improve your balance. Not flip flops or sandals, as these are bad for grip and balance.
3. Clear the clutter. Because they can't maintain their balance as well, older individuals are more likely to trip over clutter. Additionally, you should keep walking paths free to prevent tangled oxygen cords. In addition to being a trip hazard, throw rugs must to be taken down.
4. Stride steadily and gently as opposed to rapidly or at different paces. Maintaining your energy and endurance can be achieved by pacing yourself.
5. Complete heavier and more important jobs whenever you feel like it's the optimum moment for you to breathe. This may require you to reschedule some of your activities.
6. Take breaks when you NEED them and avoid pushing yourself too hard.
7. Invest in a grasping tool so you can reach objects on high shelves and pick up stuff from the floor. Breathing exercises that include bending over or raising your arms above your head will exacerbate your dyspnea.
8. To assist calm your skin, use lubricants with a water basis. You should use gauze to keep your ears and cheeks from being irritated and water-based lubricants on your lips and nose to avoid dryness because oxygen can dry up your skin, mouth, or throat.
9. Wear oxygen while engaging in exercises. When going up stairs or to the post office, many individuals forget to take off their oxygen, although these are the exact moments when your body needs oxygen the most. When you're done with your task, you can switch to a portable oxygen pack and then go back to the concentrator. You run the risk of being injured and becoming weary if you don't wear the oxygen.
10. Enter the shower with your oxygen. It's a common misconception that wearing oxygen when bathing makes bathing safer and less taxing on your body. However, using oxygen can assist you prevent getting tired during potentially taxing tasks. It can be challenging to stay locked up in a hot, muggy bathroom, so you can install a fan.
To make breathing easier, try to keep the door open, use a fan to remove air, and crack open any windows. You can save energy and prevent falls by purchasing a shower chair, which will enable you to sit down while taking a bath. Installing a detachable shower head is another option. This is particularly useful as it eliminates the need to hold your arms over your head, which is a laborious position that can also cause balance issues when taking a shower. It will be simpler and require less effort to reach every part of your body if it has a long, flexible arm.
References:
Drugs.com
LamFoundation
EveryDayHealth
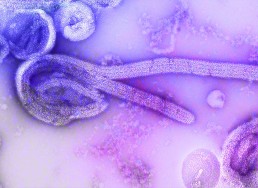
Could Ozone Therapy Combat Ebola?!
Ozone therapy is a form of alternative medicine treatment that believes to increase the amount of oxygen to the body through the introduction of ozone gas into the body. There is some evidence to suggest it can treat various diseases including cancer, AIDS, multiple sclerosis, rheumatoid arthritis, hepatitis B and C, diabetes, infected wounds, circulation disorders, and infectious diseases such as Ebola. Ozone therapy is also used for “slipped disks” in the spine, heart disease, cancer, an eye disease called macular degeneration, and Parkinson's disease. It is also used for treating abscesses and other signs of infections and is sometimes used to stop dental cavities from progressing.
Historically it has been around for a while, in 1856 ozone was first used in a health care setting to disinfect operating rooms and sterilize surgical instruments. By the end of the 19th century ozone was being used to disinfect drinking water of bacteria and viruses. In 1892 The Lancet published an article describing the administration of ozone for the treatment of tuberculosis and it was used during the First World War to disinfect wounds.
Ozone is a naturally occurring chemical that consists of three oxygen atoms. Ozone is a powerful oxidizing agent and high concentrations of ozone can be toxic to living organisms and is considered a major source of pollution. However, small ozone doses are thought to increase some naturally occurring antioxidants in the body which are thought to help to fight off cancer, viruses and bacteria and benefit the body in other ways as well.
Ozone therapy involves the introduction of ozone into the body via various methods, usually involving mixing the ozone with various gases and liquids and injecting this into the body, either via a muscle, under the skin or directly into a vein. Ozone can also be introduced via autohemotherapy, in which blood is drawn from the patient, exposed to ozone and re-injected into the patient.
However the safety of ozone has not been studied enough to know if it is safe or what side effects it might cause. Ozone is known to be toxic when inhaled from polluted air in large amounts and when given intravenously by injection, it can cause serious side effects including blood clots in the lung. Ozone produces free radicals, an over-abundance of which is known to cause oxidative stress and cell damage, and is thought to worsen some degenerative diseases. The development of hepatitis and death has also been reported.
A group of doctors who are experts on oxidative therapy have travelled to Sierra Leone as they believe that ozone therapy is an inexpensive and very safe treatment for the devastating disease, Ebola that has recently become widespread. They travelled there at the end of 2014 to teach healthcare workers to administer the treatment, even the President of Sierra Leone publicly had the treatment.
They believe that ozone is extraordinary in terms of its anti-infective and antiviral action, all that is needed is the machine and a needle, making it uncostly and it has virtually no toxic side effects, which makes it perfect for both prevention and treatment of all sorts of infections and viral afflictions, including Influenza and Ebola.
With bacteria, ozone works by puncturing the membrane of the bacteria, causing it to spill its contents and die. It also inactivates viruses, and does so 10 times faster than chlorine. It is believed that ozone is perhaps the most powerful natural oxidant in the world, and that it has the advantage of stimulating the immune system, and modulating it—either up or down depending on what your system requires.
Unfortunately the treatment being given over in Sierra Leone was stopped due to scepticism and a lack of concrete scientific evidence to back up the treatments even though there were many reported cases of infected individuals recovering from Ebola after having ozone treatment.
Hopefully more scientific studies will be carried out so as to ascertain once and for all whether ozone therapy could be used to treat a wide variety of diseases and medical complaints and could potentially in the future be a cheap, effective, low-risk, low side-effect method to treat so many different ailments and infections and become a ground-breaking discovery. It would be extraordinary if it was found to be a treatment for common widespread infections such as the Flu and Ebola and could eradicate these diseases.
References: http://www.newsmaxhealth.com and http://www.webmd.com and http://en.wikipedia.org and http://articles.mercola.com

Practical tips using oxygen
Tips For The Use Of Supplemental Oxygen
Practical Tips:
1. Keep away from any flame or spark such as gas stoves, fireplaces and candles. Even electric razors can cause sparks so do not use your oxygen whilst shaving. Oxygen isn't flammable but it is combustible and can aid in the starting of a fire.
2. Do not allow any smoking anywhere near. Some people put signs up in their homes for visitors to let them know.
3. When cooking try not to wear loose fitting clothes and stay as far away from the heated surface as possible.
4. Avoid using any aerosol products as they can ignite in the presence of a spark.
5. Do not allow flammable liquids to get on your clothing or body as unless washed thoroughly, these could become a hazard.
6. Do not place your oxygen concentrator in an unventilated area, such as a closet. Not only does the concentrator generate a lot of heat but it uses the surrounding air to produce oxygen so the oxygen in the atmosphere will quickly become depleted in small spaces.
7. Secure all cylinders to prevent them from falling over. A falling oxygen cylinder can cause damage to the valve, releasing the pressure, which may cause it to become a dangerous projectile.
8. Call your electric company to inform them that you are using oxygen. Firstly some electric companies have a program that allows a reduction of your rates to help lower the cost of running the air concentrator. Secondly, they will generally put you first in line when restoring power after an outage. They may also be able to provide specialist adaptors or devices to aid you with your mobility and medical equipment to make life easier.
9. Oxygen hoses can be a tripping hazard so try to have your concentrator in a position for maximum mobility but also where the hose will not cause you or others to trip. Use a coloured hose to make it more visible.
10. Keep the hoses clean and replace on a regular basis. Make sure the filters are replaced regularly, wipe it down with a damp cloth to remove dust and clean tubing to prevent mould if you use water to humidify your oxygen.
Ensure you have an emergency plan arranged in case there is a power outage.
• Inform your power company that you are oxygen-dependent. Many companies offer oxygen-dependent patients priority service and will inform you of upcoming maintenance/outages and ensure your power is restored as a priority.
• Collaborate with your oxygen supply company. Ask them to help you determine exactly how much oxygen you will need in case of an emergency power outage. They may also provide you with an emergency cylinder.
• Contact your local police and fire departments to let them know that you are oxygen-dependent.
• Talk to your doctor about reducing your oxygen flow rate during an emergency. This may help buy you some time and extend the life of your oxygen supply.
• Consider installing your own emergency generator, especially if you live in a remote location.
• Organize a support team of family or friends whom you can call in case of an emergency.
References:
http://blog.copdfoundation.org and http://copd.about.com and www.southern-electric.co.uk

Everyday Uses of Oxygen
Oxygen is an amazing substances that also has a variety of applications in our every day lives.
 Respiration:
Respiration:
• Every living creature and plant requires oxygen to survive.
• Oxygen therapy is prescribed for patients diagnosed with chronic obstructive pulmonary disease (COPD) as well as other medical conditions, that require oxygen to be administered at home to aid in the treatment of that condition. The use of pressurized oxygen therapy has also provided outstanding medical benefits.
• Oxygen is a standard treatment for many patients that find themselves in hospital, which have a huge supply on site.
Metallurgy:
• The production of steel is reliant upon oxygen where it is used in a blast furnace to turn carbon into carbon dioxide, which reduces the iron oxides to pure iron.
• Oxygen is also used in torches for cutting and welding. Oxygen reacts with hydrogen in which it can heat to over 5,000 degrees. These torches can cut through or weld together most metallic substances.
Rocketry:
• As a liquid, oxygen is used widely both medically and industrially, most commonly as an oxidizing agent for use in missiles and rockets where it reacts with liquid hydrogen to produce the thrust for take-off. Astronauts’ spacesuits have close to pure oxygen.
Chemical Synthesis:
• Hydrocarbons are broken apart by heating them with oxygen. This method is used to induce combustion in order to produce water and carbon dioxide. Also if the mixture is controlled it can break apart the hydrocarbons to produce acetylene, propylene and ethylene.
• Oxygen is also used at plants that treat sewage or purify water. Oxygen is pumped through water to increase the production of natural bacteria, which break down waste products.
• Oxygen as a gas is required to produce energy in industrial processes, generators and ships and it is also used in airplanes and cars.
References: http://www.ehow.com and http://www.usesof.net/uses-of-oxygen.html

Lung Conditions Shouldn't Stop You From Planning A Holiday This Summer!
There is a myth that if you are on oxygen therapy then your life is effectively over and that it is too restrictive and complicated to go away on holiday. This is not necessarily the case and for most sufferers the world is your oyster. Always check with your doctor first to ensure you are fit enough to travel and ask your doctor to write a letter stating this just in case you need it.
All you need to do is prepare and plan the holiday well and ensure that you consider some factors when planning your trip:
• Climate: many people with lung conditions prefer warm climates that have salty air. Lower oxygen levels at higher altitudes can make breathing difficulties worse.
• Terrain: whether your destination is flat or on a hill could affect your ability to get around comfortably.
• Wheelchair access.
• Transport availability.
• Special needs such as oxygen treatment.
• Plan in advance: if you leave things to the last minute, you could forget something crucial. Think about how far you can walk, how many stairs you can manage, access to toilets and what transport you can use.
• Be realistic: places you liked in the past may not be suitable now. Pick something you and your carer can cope with physically.
• Shop around: different companies have different policies for people with lung conditions, so find the best deal for you. Many travel agents offer holidays for people with special requirements.
• Ask questions: travel firms are used to dealing with special requirements. They should be able to answer all of your queries and concerns.
Arrange Insurance
You should ensure that you and your carer have full travel insurance before going away to avoid huge medical bills if you are taken ill during your trip. Look into this first as it may be expensive and you may need a specialist provider depending on your health. Check that it covers all aspects of your medical condition and that you declare everything accurately to them otherwise it may not be valid, leaving you with a huge bill.
Keep your documents safe with you while you travel in case you need them suddenly in an emergency.
The European Health Insurance Card (EHIC) entitles you to reduced cost – sometimes free – medical treatment if you fall ill when travelling in Europe.
Choosing Accommodation
Accommodation in the UK is divided into four mobility categories:
• Category One – suitable for people able to climb a flight of stairs that have extra fittings to aid balance.
• Category Two – suitable for someone who needs a wheelchair some of the time but can manage a maximum of three steps.
• Category Three – suitable for people who depend on a wheelchair but who can transfer unaided to and from the wheelchair in a seated position.
• Category Four – suitable for a person who depends on the use of a wheelchair and needs help from a carer or a mechanical hoist to transfer to and from the wheelchair.
Each category has its own logo, which is displayed by accommodation providers that have been assessed. Make sure you choose accommodation that best fits of requirements.
Other countries have different systems so just make sure you ask your travel agent about how to choose your accommodation abroad.
Getting There
Coach
Several coach companies are working towards making their vehicles accessible for people with disabilities. Many coaches now feature kneeling suspension, which makes boarding and alighting easier. Most on-board toilet facilities are now level with the coach seating.
Some companies allow you to bring on board your own oxygen supply and will carry some types of collapsible battery-powered wheelchairs.
Train
Different train companies have different policies regarding people with disabilities, so plan your route in advance and find out which companies’ trains you need.
Ferry
Many ferry companies have lifts, toilets and wheelchair facilities; some can supply wheelchairs at terminals. A few have special cabins for disabled people and/or offer discounts. Check before you book, especially if you need oxygen.
Camping and caravanning
The Camping and Caravanning Club has three stages of accessibility for camping and caravan sites. So you just need to check that the site is appropriate for your needs.
• No accessible facilities;
• Accessible to people who can move around a little, but not wheelchair accessible; and
• Fully accessible including shower blocks and facilities.
Holidaying With Oxygen
Oxygen for travel in the UK is provided by the NHS. You just need to let your usual oxygen provider know the details of your holiday, including the dates you are going and returning and where you will be staying, and they will arrange everything for you.
You should first get permission to store oxygen cylinders and equipment from the owner of the place where you are staying.
Oxygen suppliers in the UK will only provide oxygen for travel and stays within the UK. If you are travelling abroad then there are many overseas oxygen providers that can fulfil your oxygen requirements and if you are travelling by plane then you need to ensure your airline's oxygen policy and whether you need to complete any additional documentation for them.
Flying with a lung condition
Many people believe their lung condition will prevent them from flying, especially if they need oxygen but this is not necessarily true. First, ask your doctor whether you can travel by plane and whether you will need any additional oxygen on the plane.
Then contact individual airlines to discuss your requirements and to find out what their policy is for carrying and using oxygen on planes.
If you are planning a long-haul flight and use a continuous positive airway pressure (CPAP) machine to treat the sleep disorder obstructive sleep apnoea (OSA), you should consider whether you might need to use your machine during the flight.
Some airlines have restrictions on what machines are permitted for use on board and others may require you to fill in a form before you travel.
When you contact the airline, find out what assistance is available at the airport as well as on the plane and check:
• the airline’s policy on carrying and using oxygen and medical devices such as CPAP machines;
• the exact length of the flight, and whether delays are likely;
• the facilities available at the outgoing and incoming airports. These might include assistance to get you from the airport lounge to the departure gate and on to the plane, the use of wheelchairs, and whether oxygen is available at the airport; and
• how you should confirm your fitness to fly.
Medication
If you are on medication then you will need a letter from your doctor confirming that you need the medication, and you should also keep a list of all the medication and doses you take in case you need to get more during your stay. List the proper names, keep all medication in its original packaging and keep it with you in your hand luggage. A doctor’s letter is required for liquid medicines exceeding 100 millilitres that are taken into the aircraft cabin. When given medication abroad, check whether it can be brought back into the UK. If you are in any doubt, declare the medication at customs.
Preparation is the key. Plan your trip in advance, think through everything you need, ask as many questions as you can of as many people as possible, then decide what’s best for you.
References: http://www.blf.org.uk and http://www.cancerresearchuk.org

Extreme Weather Can Trigger Your Asthma

For most people, if their asthma is managed properly and under control then the weather should not have much of an effect, however for others extreme weather conditions can bring on symptoms and organisations suggest extra thought and care is taken before heading out in it.
Changes in temperature of the air within your airways can cause inflammation, for most this is not a problem as the nose controls humidity and temperature. With people who suffer from asthma, they tend to breathe more through the mouth and irritants, pollutants and pollen are more of a factor and many already have inflammed airways. The more severe the asthma, the more likely it is that the weather will affect them.
Common weather triggers include:
• Cold air can cause constriction of airways.
• Wind and rain-Rainfall can increase and stir up mould spores, and wind can blow around pollen and mould.
• Heat-increased ozone from smog, exhaust fumes, and pollutants tend to be higher. Dry hot air can also trigger asthma.
• Lightning-Thunderstorms, which can generate ozone, are now thought of as an asthma trigger.
• Air pressure fluctuations-Barometric pressure can trigger sinus episodes and sinusitis is a common asthma trigger.
Cold Winter Air:
75% of asthma sufferers say that cold air can trigger asthmatic symptoms. The advice is to ensure that you are managing your asthma and taking any prescribed medication. Just as important is to be prepared. Check the forecast and make sure you carry your inhaler with you, wrap up warm and dry and wrap a scarf around your nose and mouth and try breathing more through your nose and it will help to dehumidify and warm the air up.
Remember that the difference between inside and outside temperature can be a factor so even going in and out of heated shops, or going from a nightclub or pub out into the cold air are all times when you need to look after yourself.
Exercise is very beneficial for people with asthma as it can help improve lung function and improve fitness but over three quarters of people with asthma have told Asthma UK that exercise in colder weather is a trigger for their condition. This is mainly due to the fact that during aerobic exercise you would inhale more of the cold air, breathing it in through your mouth (which means that it is not warmed or moistened by your nose) and breathe it more deeply into your lungs.
There are many things you can do to maintain your exercise regime but avoid the triggers.
• Exercising indoors or at a gym or gym classes instead of venturing outside.
• Warm up and warm down for 10-15 mins before and after outside exercise.
• Dress appropriately with a scarf around your throat and nose.
• If symptoms begin stop exercising immediately, take your inhaler and wait until you feel better before you resume.
• Consider more moderate exercise that will reduce the need for such deep breaths like a power walk instead of a run or a more gentle bike ride.
When it is cold many avoid going outside to try and avoid the triggers, however spending more time indoors exposes you to more triggers within the home such as pet hair, smoke, dust mites, fireplaces etc. Many sufferers prepare themselves for this and from being out in the cold by having a back-up home oxygen supply to use when the cold weather has triggered off a bad asthma attack.
Thunderstorms:
More recently it has become apparent that thunderstorms can trigger serious asthma attacks, especially children and young adults, with large numbers of people needing to go to A&E.
It is not fully understood why this happens, but it is thought during a thunderstorm, the windy conditions cause high levels of pollen and mould spores to be swept up high into the air where the moisture breaks them into much smaller pieces. As the pollen and mould particles then settle back down, these smaller pieces of pollen and mould can be breathed into the smaller airways of the lungs where they irritate the airway and trigger asthma symptoms.
Not all thunderstorms trigger asthma, it seems to depend upon the time of year, the humidity, wind, air pressure and whether ozone levels are high.
The advice is to be aware of weather forecasts, try to avoid being caught outside in them and make sure you carry your inhaler.
References: http://www.everydayhealth.com/asthma and http://www.asthma.org.uk

The Truth About Oxygen Bars: Healthy Trend or Just Hype?
You may not believe this but customers pay to breathe in 40% oxygen through a plastic hose that is placed into their nostrils at oxygen bars, which first appeared in the US in the late 1990s. You may also select from a variety of oxygen flavours, like peppermint, cranberry, or even scented candles. The length of the oxygen experience varies based on the customer's budget and preferences, usually lasting between a few minutes and roughly twenty minutes.
What Are The Promises of Oxygen Bars?
Although the proprietors of oxygen bars take care not to make any medical claims, they advertise their services for leisure and rely on client endorsements. Benefits like less stress, relief from pollution, more energy and alertness, better hangover recovery and relief from headaches and sinus issues are among the many advantages that users frequently mention.
The Science of Oxygen Bars: Is It Real or Is It Hype?
Despite these assertions, there are no extensive, carefully conducted scientific studies that back up any advantages of oxygen inhalation for healthy people. According to the American Lung Association, breathing oxygen is unlikely to have any physiological advantages for healthy individuals. Conversely, there's no proof that breathing in oxygen is hazardous either.
Oxygen Bars and Health Issues
Oxygen is usually given at home under a physician's supervision to patients with illnesses that impair lung function. Medical experts advise against giving these individuals oxygen bars because each person has different oxygen needs that need to be checked and adjusted by a healthcare practitioner. Uncontrolled oxygen use may be harmful, possibly resulting in dangerous oxygen intake levels or interfering with continuing medical care.
Fears Relating to Flavoured Oxygen
The usage of flavoured oxygen is one of the main issues with oxygen bars. These flavours are produced by pushing the vaporised aroma through the hose after bubbling oxygen through bottles containing aromatic solutions. While some bars employ food-grade, oil-free particles to create the scent, others might use aroma oils. Lipoid pneumonia is a dangerous lung inflammation that can be brought on by breathing in greasy materials. The purity or sterility of the fragrances cannot be ensured, even with oil-free mediums, which presents a risk for bacteria, allergies, irritants, and other pathogens.
Furthermore, a lot of oxygen bars can be found in places where smoking is allowed, such as casinos and nightclubs. Because oxygen can fuel combustion and increase the risk of fires, this poses safety issues.
Regulation and Research Are Necessary
Before oxygen bars are considered safe for use by healthy individuals, more thorough testing, research, regulation and medical oversight are required. It is now deemed dangerous to change a patient's course of treatment for medical disorders that call for oxygen therapy. Scientific research may someday corroborate testimonies, but for the time being, the claimed advantages of oxygen bars are mostly unsubstantiated and may even be psychological.
See MedicineNet and WebMD for additional details.

Oxygen Therapy and Autism
Hyperbaric Oxygen Therapy (HBOT) has only recently in the last two years been used to treat children with autism but with amazing results.

A study in 2012 by DA Rossignol et al proved that children with autism who received hyperbaric treatment for 40 hourly sessions showed significant improvements in overall function, receptive language, social interaction, eye contact, and sensory/cognitive awareness compared to children who received just pressurized room air.
When a person concentrates on a task or to generate speech, the brain is doing more work and there is an increase in blood flow to the brain, specifically the parietal frontal cortex, which is located behind the forehead. This increase in blood flow supplies the brain with more oxygen and glucose, giving the cells their needed energy to perform their task. In autistic children the opposite happens, they have diminished blood flow to begin with, and when their brain is attempting to perform a task their blood flow does not increase and does not supply the brain with the necessary oxygen and glucose the cells need.
The theory behind using HBOT on children with autism is that the increase in oxygen will reduce excess swelling of brain tissue, increase cerebral blood flow and stimulate cerebral tissue. There are correlations linking it to being able to remove toxins, reduce inflammation allowing oxygen deprived areas to have a return of blood flow, builds new capillaries in the brain and reduces the inflammation in the gut.
The belief is that all of these results will allow the brain to do its job better, resulting in a child who is more "present" in regards to social interaction and communication.
Studies and parents have reported that autistic children showed improvement in sleep, children becoming calmer and more affectionate, improved focus and attention, improved bowel function, improved cognitive and linguistic skills, being less sensitive to noise and appearing more 'present' and 'connected' to family members.
There are some unknowns however, such as any long-term affects, whether the treatments are long-lasting or not and whether certain autistic sufferers respond better than others. HBOT is definitely not a cure but it appears to be able to help some autistic children improve their behaviour, cognitive functions and quality of life and bring them a step closer towards 'normal'.
References: http://freshstarthyperbaric.com/adhd.php and http://oxfordhbot.com/hbot-for-autism/
Could Oxygen Make You Smarter?!
Research carried out at the Human Cognitive Neuroscience unit at the University of Northumbria, have discovered that mental performance can be greatly improved by inhaling a shot of oxygen.
Our brains only account for 2% of our body weight however it consumes the most energy (20-30%) out of all the organs but yet it cannot store very much energy and relies on a constant supply via the bloodstream.
In the tests students were given a one-minute blast of oxygen after being asked to remember a list of words. They remembered more words than those who didn't take any additional oxygen. Other students took oxygen whilst they were playing the higher levels of Tetrix, a computer game and it was found that they performed much better compared to students who didn't take any additional oxygen.
It would appear that additional oxygen blasts can aid in the brain performing at an increased level while it is attempting more demanding tasks.
Dr Sholey adds; "Even the most esoteric brain functions obey biological rules. By tweaking fuel availability to the brain, simply by throwing a bit more fuel on to the fire, you can improve cognitive function to some degree."
Cognitive improvement has been recorded in patients who use oxygen therapy at home but can also be linked to the research that has been carried out that suggests exercise will make you smarter. Exercise will improve your cardiovascular system which will in turn increase the amount of oxygen being pumper round the body. The brain relies on the bloodstream for it's oxygen supply and therefore will receive the optimal amount of oxygen possible if we are at our fittest. More fuel means more energy, which results in improved brain function.
However there is also research and studies that suggest that short periods of hypoxia (oxygen deficiency) also aids in increasing and improving oxygenation levels in the body and brain and could also aid in improving brain function ability. It is thought to be the reason why so many people who live in mountainous regions (where due to the altitude the oxygen levels in the air are a lot lower) live a lot longer. It is thought that a temporary, brief state of hypoxia causes reserve capillaries to open up, increase the amount of erythrocytes in the blood, increase the amount of circulating blood and increase blood supply to tissues. It is believed to improve your mood, immunity and metabolism as well as mental and physical capabilities. The idea was tested via a mask that alternated between a gaseous mixture containing normal oxygen levels and one that contained a much lower level. A similar affect can be carried out by ourselves easily by adjusting our breathing patterns and letting out a very long exhale, which will create a temporary hypoxic state.
References: http://www.theguardian.com and http://www.intellectbreathing.com